Artiglio
Excellence in componentsLanguage: English
 |
 |
 |
 |
 |

- Zoom stereo microscope for dental labs
- Prismatic dental loupes SLH
- SLH Binocular Loupes
- SLT Binocular Loupes TTL
- SLF Binocular Loupes
- Headlighting
 Printable version
Printable version  Request informations
Request informations  Tell a friend…
Tell a friend…
| Magnification systems

Magnification systemsBorn to be used in surgery, the magnification systems have also had a great diffusion in other areas (dentistry, otolaringology, obstestrics, aesthetics, ...) above all for the growing need to accurately assess the work to be performed. |
Generally we consider MICROSCOPE and / or BINOCULAR LOUPES necessary to magnify very small things, but it is not always so.
The main function is to allow us to "distinguish" (technical term resolve) the details of extremely small structures.
The magnification of the details is a secondary feature of the instrument.
IMAGE MAGNIFIED

IMAGE MAGNIFIED AND RESOLVED
RESOLVING POWER
RESOLVING POWER is the capacity of an instrument to distinguish two points of an object which are close together, as two distinct points.
The main function is to allow us to "distinguish" (technical term resolve) the details of extremely small structures.
The magnification of the details is a secondary feature of the instrument.
IMAGE MAGNIFIED
IMAGE MAGNIFIED AND RESOLVED
RESOLVING POWER
RESOLVING POWER is the capacity of an instrument to distinguish two points of an object which are close together, as two distinct points.
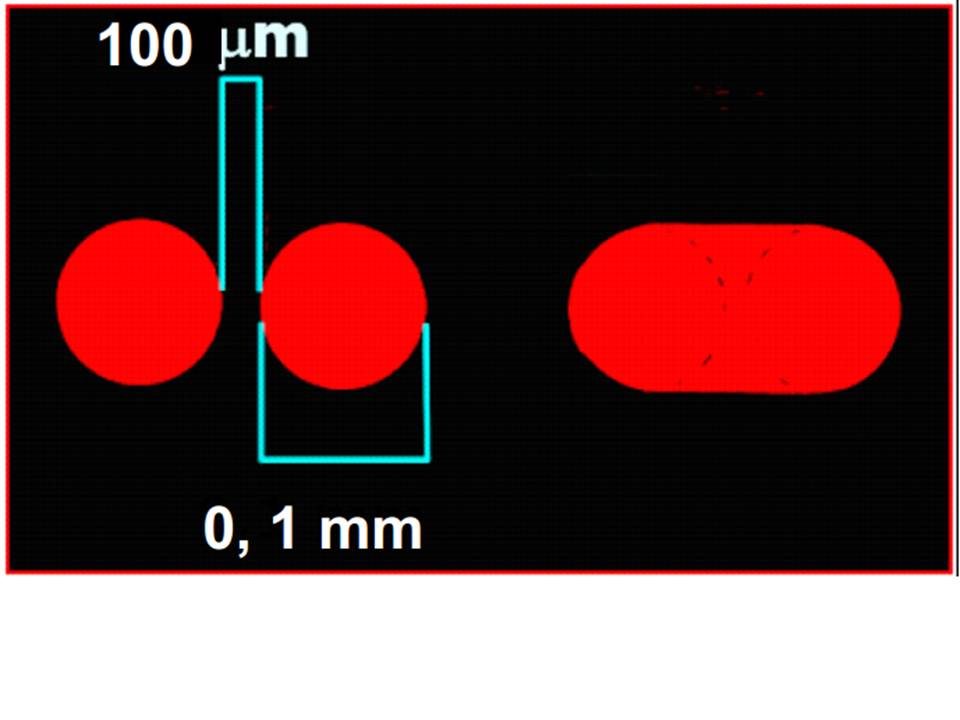
Acuity of the naked eye
THE BEST VISUAL ACUITY OF THE HUMAN EYE is 0.1 mm (100 µm), that is, the human eye cannot distinguish two separate points less than 0.1mm
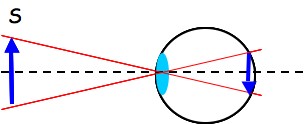
The image of an external source S on the retina increases in size as the source approaches.
However if approaching at a smaller distance of the near point (25 mm) the image is not focused sharply on the retina.
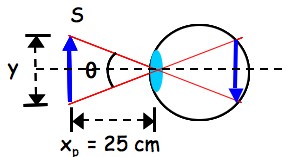
If two point sources that are at the minimum angular distance to be separately identified ( θ ), are placed in the near point (xp= 25 cm) they must be separated of at least
y = xp θ = 0.25 m 4 10-4 = 0.1 mm = 100 μm
The smallest detail tha can be appreciated by the naked eye, in the near point, has the size of 100 μm.
Picture of an external source on the retina Picture of an external source placed in the near point, on the retina
Picture of an external source on the retina Picture of an external source placed in the near point, on the retina
There are two designs for the positioning of the optics:
- TTL (Through-The-Lens), have optics that are set in the lens of the frame. The loupes are individually customised for the single user (working distance and inter-pupillary distance);

- Flip-Up, have optics that are attached to a mechanism that allows them to "flip-up" out of the way when not neede (e.g. whilst talking to the patient) and it's easier to add prescription to frame. Thanks to their versatility (adjustable pupil distance) they can be adjusted for different users.

The choice is a matter of individual preference.
Further classification can be made according to the adopted optical sysstem.
The common optical systems used are:
- GALILEAN system, consisting of a pair of lenses (positive-negative), having an excellent brightness and a wide field of view joint to smill size and extreme lightness. It is generally used for magnification up to 3,5x
- PRISMATIC system (or Keplerian), composed by a pair of lenses (positive-negative) and at least an upright prisme. The weight and dimensions increase significantly but the result is higher magnifications.

There are essentially two reasons to adopt magnification systems:
- ERGONOMIC reasons,
- OPTICAL reasons.
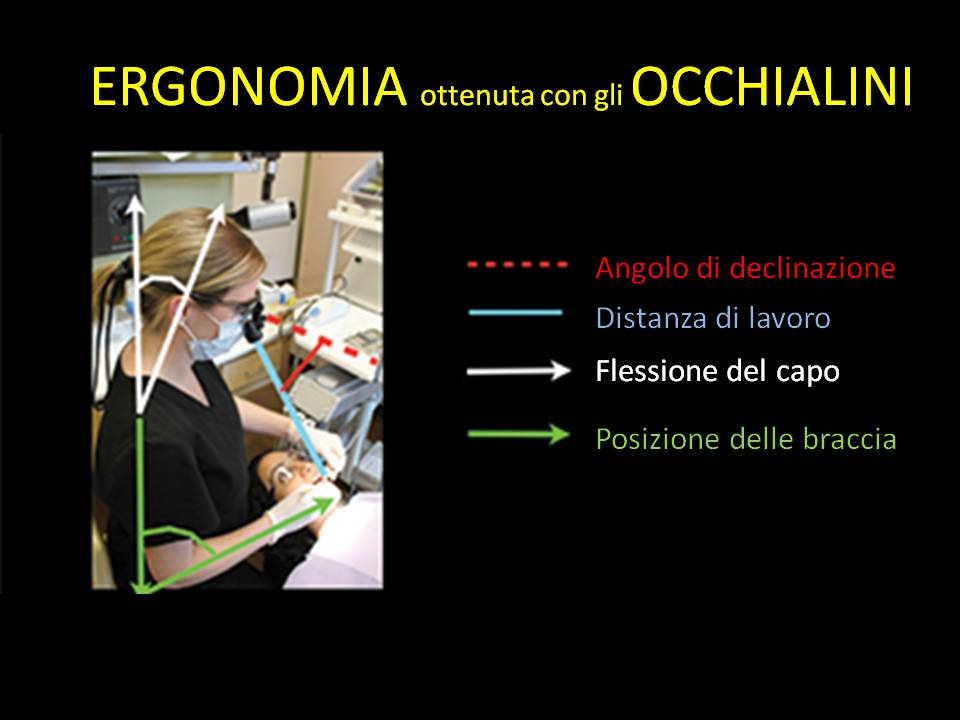
ERGONOMICS
Approximately 70% of dental professionals report one or more muscoloskeletal disorders (neck, ahoulder, lower back region).
Most pf these deseases is due to poor posture adopted during the work.
Many risk factors for work-related musculoskeletal disorders (WMSDs) can be minimized or eliminated through prevention and ergonomic strategies.
Evaluation of working postures
MSD is common in occupations that involve repetitive moements and prologed, statis postures such as sitting or standing, both of which are prerequisites to dental clinicians.
MSD is common in occupations that involve repetitive moements and prologed, statis postures such as sitting or standing, both of which are prerequisites to dental clinicians.
The posture described in "ISO Standard 11226 Ergonomics – Evaluation of static operative postures" is recommended for the dentists and is called balanced or neutral posture.
The balanced posture features can be summarized as it follows:
The balanced posture features can be summarized as it follows:
-a straight back and respect for the body symmetry; avoiding rounding the back into "C" shape;
-forward inclination of the trunk of a maximum of 20°; a greater forward inclination, the tilting to a side and the trunk rotation are contraindicated;
-forward inclination of the head up to 20-25° from the trunk;
-the arms placed along the body, forward oriented within 10°; the forearms raised up to 25° from the horizontal line;
-the angle between the thighs and shanks of 105-110° or more;
-the thighs apart up to 45°, avoiding a rigid fixation of the hip joint;
-the shanks oriented perpendicular to the floor or slightly posterior;
-the feet on the floor oriented forwards in the same plane with the shanks; when the feet are symmetrically positioned below the operator hands, the posture is balanced.
-forward inclination of the trunk of a maximum of 20°; a greater forward inclination, the tilting to a side and the trunk rotation are contraindicated;
-forward inclination of the head up to 20-25° from the trunk;
-the arms placed along the body, forward oriented within 10°; the forearms raised up to 25° from the horizontal line;
-the angle between the thighs and shanks of 105-110° or more;
-the thighs apart up to 45°, avoiding a rigid fixation of the hip joint;
-the shanks oriented perpendicular to the floor or slightly posterior;
-the feet on the floor oriented forwards in the same plane with the shanks; when the feet are symmetrically positioned below the operator hands, the posture is balanced.
Generally dental clinicians claim that they have a good view at 25-30 cm from the patient.
25 cm is in fact the NEAR POINT of human eye, ie the minimum distance at which there is a distinct image on the retina.
A normal eye is not able to focus on objects closer than 25 cm.
The distance of 25 cm, however, implies a poor posture: the operator is forced to "bend down" on the patient then making twisting of the torso and neck.
The optimal working distance in a sitting position depends on the operator's height and generally varies from 34 to 46 cm.

OPTICAL
As shown below, a magnification of 2.5x shows a clear improvement in vision of the working site.
The improvement in dignosis and operative treatment are well documented. 
2.5x magnification is stated as the standard for general dental procedures.