Artiglio
Excellence in componentsLanguage: English
 |
 |
 |
 |
 |

 Printable version
Printable version  Request informations
Request informations  Tell a friend…
Tell a friend…
| Attachments choice: rigid or resilient?

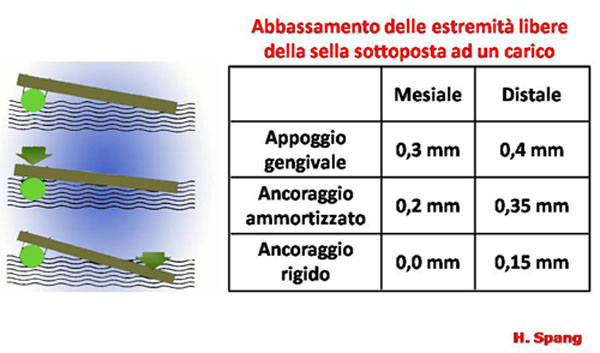
Attachments choice: rigid or resilient?Until the ‘70 people used to think that rigid connections could stress the pillar teeth more than their load capability and so they were considered dangerous; that’s why the choice was almost for resilient attachments.In the ’70 was demonstrated that the use of resilient attachments caused a series of disadvantages such as a high reabsorption of the alveolar ridges and consequent damages to the alveolus of the pillar teeth. On the opposite, the rigid attachments caused very little atrophy of the ridges and needed few reline operations. In any case the attachments choice between rigid or resilient depends basically on three factors:
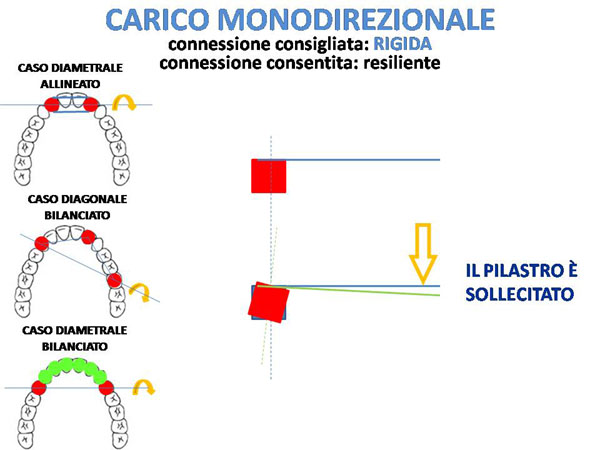
The actual orientation is to adopt rigid connexions, while in the past there where most of all resilient connexions.
In cases of prostheses with implants rigid connexions are preferred but, with traditional combined prosthesis, it is often difficult to decide how, when and why to choose a rigid connexion instead of a resilient one.
Considering that there could be different theories about the use of rigid or resilient connexions, is there any easily understandable "technical" reason to establish a reference criterion to choose which sysyem to adopt?
There are bio-mechanical reasons to determine the use of a rigid solution instead of a resilient one but, without analyse them, we can easily imagine a theoretic model made as the classic physic representation of lever degrees.
So imagine a fulcrum on which you have a segment (the lever): you apply the force on one extremity and the resistance on the other one.
Another possible representation of the system is the horizontal seesaw used by the children, who play pushing with their legs to go up and down alternately. The only different is that in our case mastication forces are applied on both the sides of the segment.
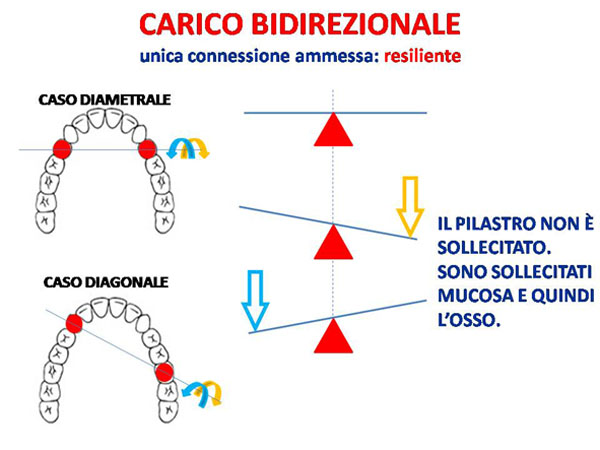
BI-DIRECTIONAL LOADthe only accepted connexion is: resilient
E’ preferibile infatti, quando la situazione lo consente, caricare gli elementi pilastro e non le parti mucose e quindi l’osso.
E’ noto infatti che le protesi ad appoggio mucoso (totali, resilienti ed ammortizzate) provocano un riassorbimento osseo da 2 a 4 più veloce delle protesi rigide.
It is better, when the situation allows it, to load the abutment elements and not the mucosa and consequently the bone. Mucosa-supported dentures (complete dentures, resilient and amortized dentures) in fact, cause a reabsorption of the bone which is 2 or 4 times faster than that of rigid prostheses.
 |